
Module 2 - Physiology
Chapter 1: Anatomy of the Cardiovascular System
Understanding the heart, blood vessels, and blood in massage therapy
The cardiovascular system is the body’s transport network. It moves oxygen, nutrients, hormones, immune cells, and heat to tissues, and it carries carbon dioxide and metabolic waste away for removal. As massage therapists, we are not diagnosing cardiovascular disease, and we are not “treating circulation” in the way medications or surgical procedures do. But we are working with a living, adapting system that responds to touch, pressure, temperature, breathing, positioning, and the client’s nervous system state. A strong anatomical foundation helps you work safely, communicate professionally, and recognize when something is outside your scope and needs referral.
Learning objectives for Chapter 1
By the end of this chapter, you will be able to:
• List the three major components of the cardiovascular system: heart, blood vessels, and blood
• Describe the basic structure of the heart, including chambers, septa, layers, and valves
• Trace the path of blood through the heart, lungs, and systemic circulation in correct order
• Differentiate arteries, arterioles, capillaries, venules, and veins by structure and function
• Identify key “great vessels” and major vessels that are commonly referenced in health histories and clinical discussions
• Explain the basic components of blood and why they matter for massage precautions
Why this matters for massage therapy
Most clients you see will not have a “cardiovascular diagnosis” in the way they might have a sprained ankle or a rash, but many will have cardiovascular risk factors, cardiovascular medications, or symptoms that overlap with cardiovascular conditions. You will also work with people whose circulation changes with stress, sleep, hydration, pain, temperature, and posture. When you understand the anatomy, you can make better decisions about:
• Positioning (especially when dizziness, shortness of breath, reflux, pregnancy, or edema is present)
• Pressure choices and pacing (especially for clients on anticoagulants or with fragile tissue)
• When to stay local versus when to avoid an area entirely (for example, suspected thrombosis)
• How to document observations accurately without drifting into diagnosis
The cardiovascular system at a glance
The cardiovascular system includes:
• The heart: a muscular pump with four chambers and four main valves
• Blood vessels: a branching network of tubes that carries blood throughout the body
• Blood: a connective tissue made of formed elements (cells and cell fragments) suspended in plasma
Together, these structures support two connected circuits:
• Pulmonary circulation: heart → lungs → heart, for gas exchange
• Systemic circulation: heart → body tissues → heart, for nutrient delivery and waste removal
The heart: location, coverings, and layers
Location and basic orientation
The heart sits in the mediastinum, the central space between the lungs. It rests on the diaphragm and tilts slightly so that the apex points down and toward the left. This is why heart sounds and chest sensations are often perceived more clearly on the left side, though individual anatomy varies.
Pericardium: the heart’s protective sac
The heart is enclosed by the pericardium, a sac that stabilizes the heart in the thorax and reduces friction. The pericardial space contains a small amount of lubricating fluid that allows the heart to move smoothly as it beats. When the pericardium is inflamed (pericarditis), movement can become painful and cardiac function can be affected. You do not diagnose pericarditis as a massage therapist, but knowing the basic anatomy helps you understand why chest pain is never something to minimize.
Layers of the heart wall
From outside to inside:
• Epicardium: the outer layer, continuous with the pericardium
• Myocardium: the thick muscular layer responsible for contraction
• Endocardium: the smooth inner lining that blood flows across
The myocardium is the engine. It’s thickness matters: the left ventricle has a much thicker myocardium than the right ventricle because it must pump blood through the entire body at higher pressure.
Heart chambers and septa
The heart has four chambers:
• Right atrium: receives deoxygenated blood returning from the body
• Right ventricle: pumps deoxygenated blood to the lungs
• Left atrium: receives oxygenated blood returning from the lungs
• Left ventricle: pumps oxygenated blood to the body
Two internal walls (septa) separate these spaces:
• Interatrial septum: between the atria
• Interventricular septum: between the ventricles
In simple terms, the right side is the “lungs side” and the left side is the “body side,” but both sides work simultaneously in a coordinated rhythm.
Heart valves: one-way traffic control
Valves keep blood moving forward. They prevent backflow when pressure changes during contraction and relaxation.
Atrioventricular (AV) valves
These sit between atria and ventricles.Tricuspid valve: between right atrium and right ventricle
Bicuspid (mitral) valve: between left atrium and left ventricle
The AV valves are supported by chordae tendineae, connective tissue “cords” that attach to papillary muscles in the ventricles. When the ventricles contract, the chordae tendineae prevent the valve leaflets from flipping backward into the atria.
Semilunar valves
These sit between ventricles and the major arteries leaving the heart.Pulmonary valve: between right ventricle and pulmonary trunk
Aortic valve: between left ventricle and aorta
They open when ventricular pressure rises during contraction and close when blood briefly pools in the cusps after contraction, sealing the valve shut.
The path of blood flow through the heart
You should be able to trace this pathway without guessing. Here is the standard flow:
• Body → superior vena cava and inferior vena cava → right atrium
• Right atrium → tricuspid valve → right ventricle
• Right ventricle → pulmonary valve → pulmonary trunk → pulmonary arteries → lungs
• Lungs → pulmonary veins → left atrium
• Left atrium → mitral valve → left ventricle
• Left ventricle → aortic valve → aorta → systemic arteries → body
Two details that often confuse students:
• Pulmonary arteries carry deoxygenated blood to the lungs (an exception to the “arteries carry oxygenated blood” shortcut).
• Pulmonary veins carry oxygenated blood back to the heart (an exception to the “veins carry deoxygenated blood” shortcut).
Coronary circulation: the heart’s own blood supply
The heart muscle needs its own oxygen supply. The coronary arteries branch from the base of the aorta and feed the myocardium. Venous blood from the heart tissue drains into coronary veins, then into the coronary sinus, and returns to the right atrium. When coronary vessels are narrowed or blocked, the myocardium can become ischemic (low oxygen) or infarct (tissue death), which is central to angina and myocardial infarction.
As a massage therapist, you do not treat coronary artery disease. But you do need to understand why:
• Chest pain and shortness of breath are red flags
• Fatigue, dizziness, and exercise intolerance can have cardiac causes
• Stress management can be a valuable supportive goal when medically appropriate
Blood vessels: structure and function from large to small
Vessels form a branching tree that changes structure as it gets farther from the heart.
Arteries and arterioles: higher pressure delivery system
Arteries carry blood away from the heart. They have thicker walls to handle higher pressure.
• Elastic arteries: large arteries (like the aorta) with elastic tissue that helps smooth out pressure changes between beats
• Muscular arteries: medium-sized arteries that distribute blood to regions and can constrict or dilate to regulate flow
• Arterioles: the smallest arteries; they create significant resistance and strongly influence blood flow into capillary beds
Arterioles are a major player in blood pressure regulation because small changes in diameter create large changes in resistance and flow.
Capillaries: exchange sites
Capillaries are microscopic vessels with very thin walls (a single layer of endothelium). This is where exchange happens:
• Oxygen and nutrients diffuse from blood into tissues
• Carbon dioxide and metabolic waste diffuse from tissues into blood
Blood moves slowly through capillaries to allow time for exchange. Capillaries form networks called capillary beds. Some tissues (like muscles and kidneys) have dense capillary networks; others (like dense connective tissue) have fewer.
Venules and veins: lower pressure return system
Venules collect blood from capillary beds and merge into veins, which return blood to the heart. Veins have thinner walls and larger diameters than arteries, and many veins—especially in the limbs—contain valves to prevent backflow.
Veins in the legs rely on several mechanisms to return blood against gravity:
• Valves to prevent backward flow
• Skeletal muscle pump: muscle contraction compresses veins and moves blood upward
• Respiratory pump: pressure changes during breathing encourage venous return
This matters in massage because clients who stand all day, sit for long periods, are pregnant, are dehydrated, or are deconditioned may have more venous pooling and may be more prone to dizziness with position changes.
The “great vessels” you should know
These vessels are commonly referenced in textbooks, health histories, and medical conversations:
• Aorta: carries oxygenated blood from the left ventricle to the body
• Pulmonary trunk and pulmonary arteries: carry blood from the right ventricle to the lungs
• Superior vena cava: returns blood from the upper body to the right atrium
• Inferior vena cava: returns blood from the lower body to the right atrium
• Pulmonary veins: return oxygenated blood from the lungs to the left atrium
Major vessels massage therapists often hear about or palpate near:
• Carotid arteries (neck): pulse point, clinically important, sensitive region
• Brachial artery (upper arm): used for blood pressure measurement
• Radial artery (wrist): common pulse point
• Femoral artery (groin region): major pulse point, deep and sensitive area
• Popliteal vessels (behind knee): important but not a common massage focus
• Dorsalis pedis and posterior tibial arteries (foot/ankle): pulse points used clinically for circulation screening
In practice, you do not need to memorize every named branch for entry-level massage. You do need to understand what “proximal,” “distal,” “arterial,” “venous,” and “capillary exchange” mean and how that affects safety decisions.
1.2. Blood: formed elements and plasma
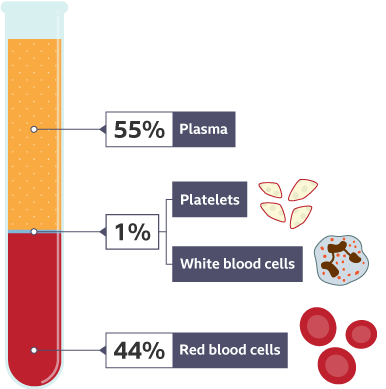
Blood is connective tissue. It is made of:
• Plasma: the liquid matrix (mostly water) carrying proteins, electrolytes, nutrients, hormones, and waste
• Formed elements: cells and cell fragments that float in plasma
Red blood cells (erythrocytes)
These carry oxygen (and some carbon dioxide) using hemoglobin, an iron-containing protein. Red blood cells are produced in red bone marrow and have a typical lifespan of about 120 days. Too few red blood cells or too little hemoglobin is anemia; too many is polycythemia, which increases blood viscosity.
Anemia may cause clients to fatigue easily, feel cold, or get lightheaded. Your role is not to diagnose anemia, but you should adjust pacing and positioning and encourage medical follow-up when symptoms are unexplained.
White blood cells (leukocytes)
These defend against pathogens and assist in immune responses. The major types include neutrophils, lymphocytes, monocytes, eosinophils, and basophils. Each has specialized immune functions.
Massage relevance: If a client has an acute infection, fever, or unexplained swelling with systemic symptoms, massage may be contraindicated or needs medical clearance, depending on the situation.
Platelets (thrombocytes)
Platelets are involved in clotting. When a vessel is damaged, clotting factors activate and fibrin forms a mesh that stabilizes a clot.
Clients on anticoagulants (“blood thinners”) or with clotting disorders bruise more easily and may have higher risk with aggressive work. This will be covered more fully in the pathology lesson, but it’s worth building the anatomical foundation now: clotting is normal and protective, but abnormal clotting can be dangerous.
Professional practice note: accuracy over myths
You will hear people say massage “flushes toxins” or “breaks up blood clots.” Those claims are not evidence-based and they create risk. Massage can support relaxation, pain modulation, body awareness, sleep, and stress reduction. It can also influence local tissue fluid dynamics and may affect autonomic tone. But clot management and cardiovascular disease treatment are medical issues.
The safest stance is:
• Be precise about what you observe
• Be modest about what massage can do
• Be confident about the value of ethical, well-reasoned touch
Quick self-check for Chapter 1
Use these prompts to test your understanding:
• Can I trace blood flow through the heart in correct order without looking?
• Can I explain the difference between pulmonary and systemic circulation in one sentence each?
• Can I describe how arteries differ from veins structurally and functionally?
• Can I name the three major components of the cardiovascular system and the four major components of blood?
• Can I explain, in plain language, why clients might feel dizzy when moving from the table to standing?
Chapter 1 Summary
• The cardiovascular system includes the heart, blood vessels, and blood.
• The heart is a four-chamber pump with layers (epicardium, myocardium, endocardium) and four major valves that maintain one-way blood flow.
• Blood flow follows a predictable path through the right heart to the lungs and the left heart to the body.
• Arteries carry blood away from the heart under higher pressure; veins return blood under lower pressure and often rely on valves and pumps (muscle and breathing) to assist return.
• Capillaries are the exchange sites where oxygen and nutrients enter tissues and waste returns to the blood.
• Blood consists of plasma plus formed elements: red blood cells, white blood cells, and platelets, each with clear relevance to safe massage practice.
Chapter 2: Physiology of Circulation
In the previous chapter, you learned the structural components of the cardiovascular system: the heart, blood vessels, and blood. Anatomy tells us what is there. Physiology explains how it works in real time. This lesson focuses on the forces that move blood, the systems that regulate circulation, and the variables that cause cardiovascular responses to change from moment to moment.
As a massage therapist, you will work with clients whose circulation adapts constantly to posture, breathing, stress, pain, temperature, hydration, medications, and activity level. Understanding cardiovascular physiology allows you to make informed decisions about pacing, positioning, pressure, and session flow while staying firmly within scope of practice.
Learning objectives for Lesson 2
• Explain how pressure gradients move blood through the cardiovascular system
• Describe systemic and pulmonary circulation in physiological terms
• Identify the factors that influence cardiac output
• Explain venous return and the mechanisms that support it
• Describe how blood pressure is regulated by neural, hormonal, and local mechanisms
• Recognize why position changes can cause dizziness or lightheadedness
• Apply cardiovascular physiology concepts to massage therapy decision-making
2.1 Circulatory pathways revisited: function, not structure
You already know the basic routes of systemic and pulmonary circulation. Here we focus on why they work.
Systemic circulation
Systemic circulation delivers oxygenated blood to tissues and returns deoxygenated blood to the heart. The left ventricle generates enough pressure to move blood through arteries, arterioles, capillaries, venules, and veins, all the way back to the right atrium.
Key physiological features:
• High pressure near the heart, decreasing as blood moves away
• Greatest resistance at the level of arterioles
• Slow flow through capillary beds to allow exchange
Systemic circulation must adapt constantly. Muscles need more blood during activity. Digestive organs need more after meals. Skin circulation changes with temperature. These adjustments happen automatically through neural and chemical signals.
Pulmonary circulation
Pulmonary circulation moves blood between the heart and lungs for gas exchange. Compared to systemic circulation, pulmonary circulation operates under much lower pressure.
Why this matters:
• The right ventricle has thinner walls because it pumps against less resistance
• Pulmonary capillaries are delicate and designed for efficient gas exchange
• Sudden increases in pulmonary pressure can be dangerous
Massage therapists do not directly affect pulmonary circulation, but breathing patterns, positioning, and relaxation influence oxygen exchange indirectly through respiratory mechanics and nervous system regulation.
2.2. Pressure gradients: the fundamental driver of blood flow
Blood moves because of pressure differences. It flows from areas of higher pressure to areas of lower pressure, just as air flows out of a balloon when released.
The heart creates pressure
When the ventricles contract, they generate pressure that pushes blood into arteries. When they relax, pressure falls, allowing chambers to refill.
Resistance shapes flow
Blood does not move freely through open space. Vessel diameter, length, and elasticity affect resistance. Small changes in arteriole diameter create significant changes in resistance and flow.
This is why arterioles are central to blood pressure regulation.
Massage relevance:
• Massage does not “push blood through arteries”
• Any circulatory changes from massage occur indirectly through nervous system shifts, muscle activity, posture, and breathing
• Understanding pressure prevents exaggerated claims and supports professional language
2.3 Cardiac output: how much blood the heart pumps
Cardiac output is the volume of blood pumped by the heart in one minute. It is calculated as:
Heart rate × stroke volume = cardiac output
Heart rate
Heart rate is influenced by:
• Autonomic nervous system activity
• Hormones (such as epinephrine)
• Fitness level
• Stress, anxiety, and pain
• Medications (for example, beta blockers)
Massage relevance:
• Relaxation-focused massage often lowers resting heart rate
• Clients on heart-rate–controlling medications may not show typical pulse responses to activity or stress
Stroke volume
Stroke volume is the amount of blood ejected with each heartbeat. It is influenced by:
• Venous return (how much blood fills the ventricles)
• Contractility of the myocardium
• Resistance in the arterial system
Massage relevance:
• Positioning and breathing influence venous return
• Gentle movement and relaxation may indirectly support efficient filling of the heart
• Overstimulation or abrupt changes can reduce tolerance in sensitive clients
2.4 Venous return: getting blood back to the heart
Venous return is a major focus in massage education because veins operate under low pressure and rely on assistance to move blood upward, especially from the lower extremities.
Mechanisms that support venous return
Venous valves
Valves prevent backflow and keep blood moving toward the heart.
Skeletal muscle pump
When muscles contract, they compress nearby veins, pushing blood forward. When muscles relax, veins refill.
Respiratory pump
Inhalation lowers pressure in the thoracic cavity and raises pressure in the abdominal cavity, encouraging blood to move toward the heart.
Gravity and position
Elevation of limbs can assist venous return, while prolonged dependent positions can increase pooling.
Massage relevance:
• Slow, rhythmic work combined with comfortable positioning supports venous return indirectly
• Clients who stand all day, sit for long periods, are pregnant, or are deconditioned may experience more venous pooling
• Sudden position changes after a session can overwhelm venous return and contribute to dizziness
2.5 Blood pressure: a dynamic variable
Blood pressure reflects the force of blood against arterial walls.
• Systolic pressure occurs during ventricular contraction
• Diastolic pressure occurs during ventricular relaxation
Blood pressure fluctuates constantly in response to posture, emotional state, hydration, activity, medications, and nervous system input.
2.6 Short-term regulation: neural control
Autonomic nervous system (ANS)
Sympathetic activation
• Increases heart rate
• Increases contractility
• Constricts many blood vessels
• Raises blood pressure
Parasympathetic activation
• Decreases heart rate
• Supports recovery and restoration
• Has minimal direct effect on vessel diameter
Baroreceptors
Baroreceptors in the carotid sinuses and aortic arch detect pressure changes and adjust heart rate and vessel tone accordingly.
Massage relevance
Massage is best understood as influencing cardiovascular physiology primarily through parasympathetic activation and reduced sympathetic tone, not through mechanical effects on blood vessels.
• Rapid positional changes can provoke baroreceptor-mediated drops in blood pressure
• Slow transitions reduce dizziness and faintness
• Conservative neck work is essential for safety and professionalism
2.7 Long-term regulation: hormonal mechanisms
Renin–angiotensin–aldosterone system (RAAS)
Low blood pressure or volume triggers renin release from the kidneys, initiating vasoconstriction and fluid retention.
This system is influenced by:
• Kidney function
• Hydration
• Chronic stress
• Medications
Understanding this system explains why hydration status and medication history matter when assessing postural tolerance and blood pressure responses.
2.8 Local regulation: endothelial function
The endothelium actively regulates vessel tone through chemical signaling, including nitric oxide release, which promotes vasodilation.
Endothelial health is influenced by:
• Physical activity
• Inflammation
• Metabolic health
• Smoking
• Chronic stress
Massage may support endothelial health indirectly through stress reduction. Observable changes such as warmth or redness reflect local vascular responses, not systemic cardiovascular changes.
2.9 Orthostatic hypotension: a common post-massage response
Orthostatic hypotension is a common post-massage event, not a rare complication.
It occurs when blood pressure drops upon standing due to:
• Venous pooling
• Delayed baroreceptor response
• Dehydration
• Medications
• Deconditioning
Massage relevance:
• Always allow time for clients to transition gradually
• Encourage seated grounding before standing
• Monitor clients at higher risk, including older adults and those on antihypertensive medications
2.10 Integrating physiology into massage practice
Understanding cardiovascular physiology allows massage therapists to:
• Select safe and effective positioning
• Pace sessions appropriately
• Use accurate, ethical language
• Document observations without overclaiming
• Recognize when referral is appropriate
Massage works with cardiovascular physiology. It does not override it.
Explicit myth correction
Massage does not detoxify blood, clear arteries, or mechanically move blood through the arterial system. Its effects occur through nervous system modulation, muscle activity, breathing, and positioning.
Chapter 2 Self-check
• Can I explain venous return without using inaccurate metaphors?
• Can I distinguish observed effects from measurable physiological changes?
• Can I explain why dizziness may occur after massage?
• Can I describe massage effects without overstepping scope?
Professional practice note
Clinical credibility comes from understanding limits as well as effects. Clear physiology supports confident communication without exaggeration.
Chapter 2 summary
• Blood flow depends on pressure gradients and resistance
• Cardiac output reflects heart rate and stroke volume
• Venous return relies on valves, muscle activity, breathing, and position
• Blood pressure regulation involves neural, hormonal, and local mechanisms
• Orthostatic hypotension is a common post-massage consideration
• Massage influences circulation indirectly and ethically
Chapter 3: Cardiovascular Pathologies, Medications, Contraindications, and Clinical Red Flags
Learning objectives
• Identify common cardiovascular pathologies encountered in massage practice
• Understand how cardiovascular medications affect massage responses
• Distinguish absolute contraindications from precautions
• Recognize cardiovascular red flags that require referral
• Adapt massage techniques based on cardiovascular considerations
• Communicate professionally with clients and healthcare providers
3.1. Understanding cardiovascular disease in context
Cardiovascular disease is not a single condition. It is a broad category that includes structural, electrical, vascular, and metabolic disorders. Many clients are stable, medically managed, and appropriate for massage with thoughtful modifications.
Key principles
• Diagnosis alone does not determine massage suitability
• Stability, control, and symptom presentation matter more than labels
• Medications often influence massage responses as much as the condition itself
3.2. Hypertension
Overview
Hypertension is a sustained elevation of arterial blood pressure. It is one of the most common conditions encountered in massage practice and is frequently asymptomatic.
Physiological considerations:
• Increased vascular resistance
• Increased workload on the heart
• Altered baroreceptor sensitivity over time
Massage considerations
Massage is not automatically contraindicated for hypertension.
Clinical priorities
• Determine whether blood pressure is controlled
• Be aware of medication effects
• Avoid abrupt positional changes
• Favor slower pacing and moderate pressure
Massage may support relaxation and parasympathetic activation, which can be beneficial for stress-related contributors to hypertension.
When to use caution or refer
• Uncontrolled hypertension
• Symptoms such as severe headache, chest pain, or dizziness
• Client reports skipping prescribed medications
3.3. Atherosclerosis and arteriosclerosis
Overview
Atherosclerosis involves plaque buildup within arterial walls, while arteriosclerosis refers more broadly to arterial stiffening. These conditions often coexist.
Physiological considerations:
• Reduced arterial elasticity
• Altered blood flow dynamics
• Increased risk of ischemia
Massage considerations
Massage does not dislodge plaque. However, conservative clinical reasoning remains appropriate.
Best practices
• Avoid excessive compression over major arteries
• Emphasize comfort, relaxation, and circulation-supportive positioning
• Monitor client tolerance and fatigue
When to refer
• New onset exertional chest pain
• Leg pain suggestive of peripheral arterial disease
• Non-healing wounds or significant skin color changes
3.4. Coronary artery disease and angina
Overview
Coronary artery disease reduces oxygen supply to heart muscle. Angina pectoris presents as chest discomfort related to exertion or stress.
Massage considerations:
• Stable, medically managed clients may safely receive massage
• Sessions should emphasize relaxation, not stimulation
• Avoid techniques that provoke breath-holding or strain
Red flags
Immediate referral is required if a client experiences:
• Chest pain during a session
• Pain radiating to jaw, neck, or arm
• Shortness of breath, nausea, or sweating
Massage therapists do not diagnose cardiac events. They recognize patterns and respond appropriately.
3.5. Heart failure
Overview
Heart failure occurs when the heart cannot pump efficiently enough to meet the body’s demands. It may involve left-sided, right-sided, or combined dysfunction.
Physiological considerations:
• Fluid retention
• Reduced exercise tolerance
• Increased fatigue
Massage considerations
Massage may be appropriate for stable clients with medical clearance.
Adaptations include:
• Semi-reclined positioning
• Shorter sessions
• Gentle pacing
• Avoidance of techniques that increase venous return abruptly
Peripheral edema should be approached conservatively and never aggressively compressed.
3.6. Arrhythmias
Overview
Arrhythmias involve abnormal heart rhythms. Some are benign; others are clinically significant.
Massage considerations:
• Many clients live normally with arrhythmias
• Medications often regulate rhythm and rate
• Massage should avoid overstimulation
Red flags
Refer if a client reports:
• New onset palpitations
• Dizziness or fainting
• Irregular pulse accompanied by symptoms
3.7. Venous disorders: varicose veins, thrombophlebitis, and DVT
Varicose veins
Dilated superficial veins resulting from valve insufficiency.
Massage considerations:
• Gentle work around affected areas
• Avoid direct deep pressure on compromised veins
• Support comfort and positioning
Thrombophlebitis and deep vein thrombosis (DVT)
These are absolute contraindications for massage over the affected area.
Red flags include:
• Unilateral leg swelling
• Warmth and redness
• Deep ache or tenderness
Suspected DVT requires immediate medical referral.
3.8. Stroke and transient ischemic attack (TIA)
Overview
Stroke results from interrupted blood supply to brain tissue. TIA involves temporary neurological symptoms without permanent damage.
Massage considerations:
• Massage may be appropriate post-stroke with medical clearance
• Sessions should accommodate sensory changes, tone alterations, and fatigue
• Communication and pacing are critical
Red flags
• Sudden weakness
• Facial drooping
• Speech difficulty
These require emergency response.
3.9. Cardiovascular medications and massage implications
Medications often influence massage responses more than diagnoses.
Common medication classes
Beta blockers
• Lower heart rate and blood pressure
• Reduce exercise tolerance
Calcium channel blockers
• Lower blood pressure
• May cause dizziness or edema
Diuretics
• Reduce fluid volume
• Increase dehydration risk
Anticoagulants
• Increase bruising and bleeding risk
3.10. Absolute contraindications vs precautions
Absolute contraindications
• Active DVT or thrombophlebitis
• Unstable angina
• Recent myocardial infarction or stroke without clearance
• Severe, uncontrolled hypertension
Precautions
• Controlled hypertension
• Stable heart disease
• Medically managed arrhythmias
• History of cardiovascular events
Clinical reasoning determines adaptation, not blanket avoidance.
Massage implications
• Monitor position changes carefully
• Use pressure conservatively
• Document medication-related observations
3.11. Cardiovascular red flags: when to refer
Massage therapists should refer when clients present with:
• Chest pain
• Shortness of breath at rest
• Sudden dizziness or fainting
• New or worsening edema
• Unexplained fatigue
• Irregular pulse with symptoms
Referral is not failure. It is ethical practice.
3.12. Communicating with clients and providers
Professional communication includes:
• Clear intake questions
• Neutral, non-alarming language
• Accurate documentation
• Respect for scope of practice
Examples of appropriate language:
• “I’m noticing something that may need medical input.”
• “Massage may not be appropriate today; I recommend checking with your provider.”
3.13 Integrating cardiovascular pathology into massage practice
Massage therapy does not treat cardiovascular disease. It supports the person living with it.
A well-informed therapist:
• Recognizes patterns
• Adapts sessions intelligently
• Communicates clearly
• Knows when not to proceed
This is clinical maturity.
Professional practice note
Authority in massage therapy comes from restraint as much as confidence. Knowing when to modify or refer builds trust with clients and healthcare providers alike.
Chapter 3 summary
• Cardiovascular disease exists on a spectrum of stability
• Medications significantly influence massage responses
• Most cardiovascular conditions are precautions, not contraindications
• DVT and unstable cardiac conditions are absolute contraindications
• Red flags require referral, not technique changes
• Ethical massage practice relies on clinical reasoning
Chapter 4: Massage Techniques and Session Design for Cardiovascular Considerations
Learning objectives
• Design massage sessions appropriate for clients with cardiovascular considerations
• Select techniques based on physiological tolerance rather than routine
• Modify pressure, pace, and positioning to support safety
• Recognize when technique adaptation is insufficient and referral is needed
• Communicate accurately about massage effects without exaggeration
4.1. Reframing “massage for circulation”
A necessary course correction
Massage education has historically framed certain techniques as “circulatory” by default. This framing often implies direct mechanical effects on blood flow that are not physiologically accurate.
Critical clarification:
Massage does not significantly increase arterial blood flow, lower plaque burden, or mechanically move blood through the cardiovascular system. Observable effects such as warmth, redness, or a sense of “flow” reflect local vascular responses and nervous system modulation, not systemic cardiovascular change.
This does not make massage ineffective. It makes precision in language essential.
4.2. What massage can influence safely
Massage may influence cardiovascular function indirectly, primarily through:
• Autonomic nervous system regulation
• Skeletal muscle relaxation
• Breathing patterns
• Postural changes
• Perceived stress reduction
These influences vary by individual and by session. They are supportive, not corrective.
4.3. Session design: the cardiovascular lens
Intake considerations
A cardiovascular-informed intake looks beyond diagnosis.
Key questions include:
• How stable is the condition?
• What medications are being taken, and when were they last adjusted?
• Does the client experience dizziness, shortness of breath, or fatigue?
• How does the client respond to position changes?
Bias check:
Avoid assuming that a “controlled” condition means predictable responses. Controlled simply means medically managed, not identical day to day.
Session pacing
Clients with cardiovascular considerations often tolerate slower pacing better than intensity changes.
Clinical reasoning:
• Rapid transitions increase autonomic demand
• Long pauses allow baroreceptor adjustment
• Gradual rhythm supports nervous system regulation
Massage sessions designed for cardiovascular safety are often quieter, slower, and less technique-dense.
4.4. Pressure: moderation over intensity
Pressure is not dose-dependent medicine
Another common bias is equating deeper pressure with greater physiological effect. For cardiovascular considerations, this is often counterproductive.
Guidelines:
• Use the minimum effective pressure
• Avoid sustained compression over major vessels
• Monitor client breathing and facial tone continuously
Clients on anticoagulants or with fragile vasculature bruise more easily, even with moderate pressure.
4.5. Positioning: one of the most powerful tools you have
Positioning influences venous return, cardiac workload, and autonomic response more reliably than any single technique.
Supine positioning
• May provoke dizziness in clients with orthostatic intolerance
• Requires slow transitions
Prone positioning
• Can increase cardiac workload in some individuals
• May be poorly tolerated by clients with heart failure or respiratory compromise
Side-lying and semi-reclined positions
• Often best tolerated for cardiovascular conditions
• Support breathing and venous return
Bias check
Do not default to supine or prone simply because they are standard. Cardiovascular physiology should inform positioning decisions.
4.6. Technique selection through a cardiovascular lens
Effleurage
Often described as “circulatory,” effleurage is better understood as:
• Supporting parasympathetic tone
• Encouraging client comfort and body awareness
• Facilitating tissue warming locally
Use long, unhurried strokes with consistent pressure.
Petrissage
Petrissage engages skeletal muscle and connective tissue.
• Avoid aggressive kneading in clients with vascular fragility
• Use intermittently rather than continuously
• Monitor fatigue
Petrissage may support comfort and muscle tone but does not “pump” blood systemically.
Compression techniques
Compression can increase intravascular pressure locally.
• Avoid sustained compression in clients with venous disease
• Use light, rhythmic compression only when appropriate
• Never apply compression over areas of known thrombosis
Tapotement and brisk techniques
These techniques increase sympathetic stimulation.
Bias correction:
Tapotement is not appropriate for many clients with cardiovascular conditions and should not be framed as a default circulatory technique.
4.7. Breathing and cardiovascular tolerance
Breathing patterns influence venous return and autonomic regulation.
Massage-relevant considerations:
• Encourage natural, unforced breathing
• Avoid cues that induce breath-holding
• Observe breathing rather than controlling it
Diaphragmatic movement supports the respiratory pump, but instruction should remain gentle and optional.
4.8. Managing post-massage transitions
As discussed in Lesson 2, orthostatic hypotension is common after massage.
Best practices:
• Allow seated rest before standing
• Offer water without implying detoxification
• Encourage slow movements
Bias check
Dizziness after massage is not evidence of “release” or “toxins leaving the body.” It reflects normal cardiovascular adjustment.
4.9 When technique modification is not enough
Massage therapists must recognize when adaptation is insufficient.
Do not proceed if a client experiences:
• Chest pain
• Shortness of breath at rest
• New or worsening edema
• Sudden dizziness or fainting
Referral is the correct response.
4.10. Communicating effects accurately
Professional credibility depends on language.
Avoid statements such as:
• “This will improve your circulation”
• “Massage helps your heart work better”
Prefer language such as:
• “Many people find massage supports relaxation and comfort.”
• “We’ll pace this session based on how your body responds today.”
4.11 Integrating cardiovascular awareness into long-term practice
A cardiovascular-informed therapist:
• Designs sessions intentionally
• Observes continuously
• Adjusts without defensiveness
• Documents objectively
• Refers appropriately
This is not limitation. It is professionalism.
Chapter 4 Summary
• Massage affects cardiovascular function indirectly, not mechanically
• Session design matters more than technique selection
• Positioning and pacing are primary safety tools
• Moderate pressure is generally safer than intensity
• Orthostatic responses are common and manageable
• Ethical communication protects both client and therapist
